
Nadia Kruger
What is Plastic Surgery?
The word “plastic” finds its origin in the Greek word “plastikos”, meaning “to mould or give form”. Thus, one can infer that plastic surgery relates to the reconstruction of body tissues, whether cosmetic or in correction of physical defects. The goal of plastic surgery is to improve function and/or appearance by operating on the skin, facial skeleton and congenital anomalies (e.g. cleft palate and cleft lip).1

Figure 1: Reconstructive surgery being performed.2
Figure 2: An engraving from “On the Surgery of Mutilation by Grafting” (1597) by Gaspare Tagliacozzi.2
Notable Journals in the Field
| Journal Name | Website |
| Plastic and Reconstructive Surgery | https://journals.lww.com/plasreconsurg/pages/default.aspx |
| Annals of Plastic Surgery | https://journals.lww.com/annalsplasticsurgery/pages/default.aspx |
| European Journal of Plastic Surgery | https://link.springer.com/journal/238 |
| Journal of Hand Surgery | https://www.jhandsurg.org/ |
Journal in the Spotlight: Plastic and Reconstructive Surgery
 Plastic and Reconstructive Surgery” publishes articles with the latest research regarding surgical techniques and patient follow-up in plastic surgery, which includes reconstruction of the maxillofacial skeleton and breast, burn repair, hand and microsurgery, cosmetic surgery and more. This journal has been publishing articles on a monthly basis since 1946, and is one of the leading reference journals for specialists and other health care professionals in the field of plastic surgery.
Plastic and Reconstructive Surgery” publishes articles with the latest research regarding surgical techniques and patient follow-up in plastic surgery, which includes reconstruction of the maxillofacial skeleton and breast, burn repair, hand and microsurgery, cosmetic surgery and more. This journal has been publishing articles on a monthly basis since 1946, and is one of the leading reference journals for specialists and other health care professionals in the field of plastic surgery.
Article Reviews
A Surgical Fix for Getting Cold Feet (or Hands) – Surgical Management for Raynaud’s Phenomenon
Raynaud’s Phenomenon is a condition characterised by the narrowing of blood vessels in the extremities (particularly the fingers) due to cold exposure or stress, which leads to ischaemia of the affected extremity.4-5 When present in the fingers, this condition can present with pallor and cyanosis of the digits, but may later present with pain, ulcers and gangrene. This condition is often associated with connective tissue disorders, particularly systemic lupus erythematosus (SLE) and systemic sclerosis (SSc). Pharmaceutical treatment is available for Raynaud’s, but surgery is indicated when the condition is irresponsive to medical treatment. However, no standardized surgical procedure has been proposed, and the outcomes of such procedures are uncertain.5
Dr Chen from Taiwan designed and proposed a procedure based on the following facts obtained from prior research findings:5
- Arteries/arterioles are innervated by sympathetic nerve fibres that stimulate these vessels to constrict; thus, peri-arterial adventitectomy of these nerves should logically improve Raynaud’s Phenomenon by removing the offending stimulus
- The nerve of Henlé, a branch of the ulnar nerve, provides sympathetic innervation to the ulnar artery.
- Ulnar tunnel release (a procedure indicated for ulnar compressive neuropathy at the wrist) also helps improve distal circulation in Raynaud’s Phenomenon.
Thus, this proposed procedure involves the neurectomy of the nerve of Henlé, along with ulnar tunnel release and ulnar, radial, common and proper digital artery adventitectomy, to result in what the author hypothesised would produce better results than that of simple peri-arterial adventitectomy.5
This study included 19 patients with 20 affected hands. These patients were all diagnosed with either primary or secondary Raynaud’s Phenomenon by a rheumatologist and hand surgeon. Patients with secondary Raynaud’s usually had underlying systemic diseases such as SLE and SSc.5
The main tool used to assess and measure the effectiveness of the procedure was indo-cyanine green (ICG) angiography, along with questionnaires to assess subjective outcomes. Each patient underwent two IGG angiographies: preoperatively (after induction of anaesthesia, before incising) and postoperatively (after loose closure of the incisions). ICG angiography was used to measure the level of perfusion of the digits prior to and after the procedure, in order to assess the level of improvement of circulation. These measurements were performed on the index, middle and ring fingers, since these digits tend to be the most symptomatic in Raynaud’s Phenomenon.5
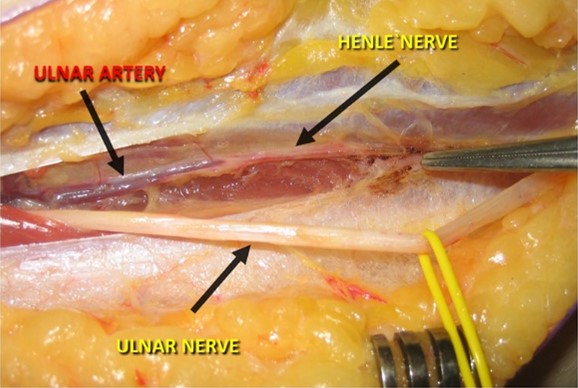
Figure 3: Intraoperative indication of a type I nerve of Henlé.6
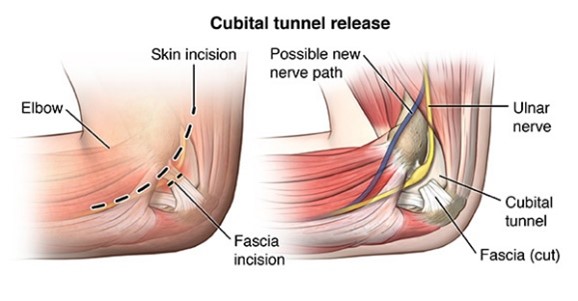
Figure 4: Demonstration of ulnar tunnel release (also known as cubital tunnel release).7
The mean ICG ingress values for the index (P = 0.03), middle (P = 0.08) and ring finger (P = 0.04) showed significant improvement in the perfusion of these digits (even though the results for the middle finger are not statistically significant, as indicated by the P-value). The mean ICG ingress rates for the index (P = 0.01), middle (P = 0.04) and ring finger (P = 0.03) also showed significant improvement.5
Long-term results, as investigated by symptom assessment annually for the three-year follow-up period, also indicate significant improvement, as shown by the following findings:5
- Decreased ulcers.
- Increased temperature of the skin of the digits (due to increased blood flow).
- Decreased pain.
The subjective assessments via questionnaires also showed notable improvements in the following areas after the three-year follow-up period5:
- Overall hand function.
- Daily activities.
- Function at work.
- Pain
- Visual appearance.
- Patient fulfilment.
- Mental health.
- Emotional experience.
- Wellbeing and health.
- Social wellbeing.
Though some patients still experienced some attacks of discolouration and pain after the procedure, these attacks dissipated swiftly. This surgical procedure helped improve the quality of life of patients involved in this study, even patients with underlying SLE or SSc.5 Longer follow-up may be necessary to assess true long-term outcomes, and the assessment of a larger cohort of patients would strengthen the author’s claims and the validity of this procedure.
Cat got your tongue? Don’t worry, you have options! – PAP vs ALT Flaps in Glossectomy Patients
Patients presenting with oropharyngeal tumours, specifically in the tongue, often need to undergo a gruelling procedure: a glossectomy. This seemingly medieval torture is often the only hopes of cure for these patients. Thus, reconstructive surgery is the only hope of any semblance of quality of life, seeing as these patients struggle with swallowing and speech, and are at high risk of aspiration. Conservation of mobility and volume replacement are the main goals of this reconstructive surgery.9
The standard flap used in reconstructive surgery of the tongue is the Anterolateral Thigh (ALT) flap. This flap usually provides sufficient soft-tissue mass and adequate pedicle length. It also allows for the inclusion of the vastus lateralis muscle, when muscular tissue is needed. This flap can also be neurotised, meaning nervous tissue can be supplied to this flap, improving speech and swallowing abilities
Unfortunately, the ALT flap has its drawbacks: It tends to have unpredictable anatomic variations in terms of vascularity, and often lacks sufficient perforators in some patients. In addressing these problems, the Profunda Artery Perforator (PAP) flap (found closer to the inner thigh) has gained popularity. This flap supplies a greater volume of subcutaneous tissue (especially adipose tissue), and is characterised by more consistent vascular anatomy. The skin is also thinner and more pliable.9
Since the PAP flap has been popularized recently, indications, volume changes, advantages and disadvantages have not been explored in comparison with the ALT flap.9 In this study, researchers explored differences and similarities between the two flaps, hypothesising that there will be no difference between the two in volume changes, functional outcomes or complications (of both donor- and recipient-sites), but that the PAP flap may provide more volume than the ALT flap.9
Patients who received reconstructive surgery for subtotal or total glossectomies between the years of 2016 to 2020, using either the PAP or ALT flaps, at the Department of Plastic and Reconstructive Surgery, University of Texas MD Anderson Cancer Center, were included in this retrospective study.9
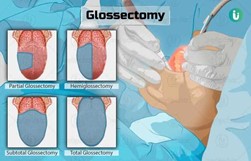
Figure 5: Images indicating the different types of glossectomies.10
What is a “flap”?
“A strip of tissue dissected away from the underlying structures but left attached at one end so that it retains its blood and nerve supply in a pedicle.”11
What is a “perforator”?
“A vessel perforating an envelope of a targeted tissue to be transferred; the superficial fascia for skin, the periosteum for bone, the perineurium for nerve, and the deep fascia for muscle.”12
Analysis was conducted by volume assessment and patient-reported outcomes:
- Volume and change of volume were assessed using computed tomography (CT) images in the axial, coronal and sagittal planes. These images were reviewed by two independent reviewers. The flap volume was determined by the measurement of five different locations along the flap, and mean measurements from each view were calculated. These measurements were used to calculate the flap volume. Two different measurements were taken at different points in time after surgery.
- Patient-reported outcomes were assessed via a quality-of-life assessment questionnaire, and a speech and swallow function assessment by a certified speech-language pathologist. Speech function was assessed by asking the patient to read a standardised passage and measuring the percentage of words intelligible to the speech pathologist. Swallow function was assessed by a modified barium swallow.9
65 patients underwent either subtotal or total glossectomies and received reconstruction, of which 46 patients received the ALT flap, and 19 the PAP flap.9 Patients who received the PAP flap generally had a lower BMI than those who received the ALT flap (22.7 ± 5.0 vs 25.8 ± 5.1; P = 0.014).9 Patients who received ALT flaps underwent similar amounts of radiation as patients who received the PAP flaps, but patients receiving ALT flaps generally received more adjuvant chemotherapy (P = 0.039).9
P = What?
The P-value indicates the validity of a hypothesis or statement on a statistical basis.14
A good way to think about it is “what is the likelihood that this result is due to chance?”, chance being something other than that which the researcher is measuring.14
Thus, P = a measure of causality, or a measure of statistical significance.
A value of P < 0.05 is deemed statistically significant.
Though the volume decrease did not differ significantly (P = 0.931) between the ALT and PAP flaps, it was found that the volume of the first measurement was significantly associated with the volume of the second measurement, i.e. both flaps shrink similarly: an increase in initial flap volume of 1cc was associated with an increase in final volume of 0.5cc (P < 0.001).9 There was no significant change between the ALT and PAP flap volumes over time, regardless of radiation therapy, proton therapy or chemotherapy exposure.9
Objective assessment revealed that patients who received PAP flaps had better swallowing abilities than patients who received ALT flaps (P=0.034) due to the higher level of pliability and greater volume of the PAP flap, however, both PAP and ALT flaps performed similarly in speech analysis, though this assessment is not statistically significant (P=0.79).9 Donor-site and recipient-site complication rates were similar for both ALT and PAP flaps, and there were no flap losses.9
The general finding of this study is that the PAP flap is a good alternative to the ALT flap, and that a lower patient BMI is the main indicator for this flap, due to the generally larger volume of this flap – patients with higher BMIs generally have sufficient volume and adipose tissue in the lateral thigh, and an ALT flap would thus provide sufficient volume, but this area is thinner and more devoid of adipose tissue in patients with lower BMIs, making the PAP flap a more attractive option.9 However, BMI is not the only indicator for this flap; deficits requiring larger volume (such as for total glossectomies) may also benefit from the PAP flap.9 The other benefits of the PAP flap as listed above are still found to be true. However, if one were to include muscle in the flap, an ALT flap is the better option: the adductor magnus muscle in the PAP flap reduces pedicle length, making this flap less ideal.9
Overall, the ALT and PAP flap are comparable in function, and are equally effective choices in reconstruction of the tongue. Differences are mainly in the indications for each flap, seeing as each has its positive and negative characteristics.
Acknowledgements
This article was brought to you by the TSSS Research Sub-Committee of 2024. The principal author of the piece is Nadia Kruger, with chief editor Catherine Joseph overseeing quality.
Bibliography
- Johns Hopkins Medicine [Internet]. Overview of Plastic Surgery. The Johns Hopkins University, The Johns Hopkins Hospital, and Johns Hopkins Health System; [cited 2024 June 17]. Available from: https://www.hopkinsmedicine.org/health/treatment-tests-and-therapies/overview-of-plastic-surgery
- Wikipedia [Internet]. Plastic surgery. Wikipedia; [updated 2024 June 13; cited 2024 June 17]. Available from: https://en.wikipedia.org/wiki/Plastic_surgery
- Plastic and Reconstructive Surgery [Internet]. About the Journal. The American Society of Plastic Surgeons; [cited 2024 June 17]. Available from: https://journals.lww.com/plasreconsurg/Pages/AbouttheJournal.aspx
- National Institute of Arthritis and Musculoskeletal and Skin Diseases [Internet]. Raynaud’s Phenomenon. National Institute of Arthritis and Musculoskeletal and Skin Diseases; [updated 2021 May; cited 2024 June 19]. Available from: https://www.niams.nih.gov/health-topics/raynauds-phenomenon
- Chen SH, Lien PH, Lee CH, Huang RW, Hsu CC, Lin CH, et al. Neurectomy of the Nerve of Henle Associated with Periarterial Sympathectomy for Management of Intractable Raynaud Phenomenon. Plast Reconstr Surg. 2024 July; 153 (6):1333-1344.
- Jengojan SA, Isaac A, Schmidhammer UPR, Tsolakidis DS, Bodner G [Internet]. High-resolution Ultrasound Visualization of Henle`s Nerve (Palmar Cutaneous Branch of the Ulnar Nerve); Normal and Preliminary Pathological Findings. European Society of Radiology; [cited 2024 June 19]. Available from: https://epos.myesr.org/posterimage/esr/ecr2020/157293/mediagallery/864138?deliveroriginal=1
- Brain & Spine Centre [Internet]. Ulnar Nerve Decompression At The Elbow. Brain & Spine Centre; [cited 2024 June 19]. Available from: https://www.brainspinecentre.com.au/ulnar-nerve-decompression-at-elbow.html
- Lim ZY, Mohan S, Balasubramaniam S, Ahmed S, Siew CCH, Shelat VG. Indocyanine green dye and its application in gastrointestinal surgery: The future is bright green. World J Gastrointest Surg. 2023 Sep 27; 15(9):1841-1857
- Ismail T, Padilla P, Kurlander DE, Corkum JP, Hanasono MM, Garvey PB, et al. Profunda Artery Perforator Flap Tongue Reconstruction: An Effective and Safe Alternative to the Anterolateral Thigh Flap. Plast Reconstr Surg. 2024 June; 153(6):1191e-1200e
- Pandey A [Internet]. Glossectomy. Myupchar Digital Hospital; [updated 2020 May 20; cited 2024 June 20]. Available from: https://www.myupchar.com/en/surgery/glossectomy
- Martin EA, Law J, editors. Concise Medical Dictionary. 10th ed. New York: Oxford; 2020.
- Yamamoto T, Yamamoto N, Kageyama T, Sakai H, Fuse Y, Tsuihiji K, Tsukuura R. Definition of perforator flap: what does a “perforator” perforate? Glob Health Med. 2019 Dec 31;1(2):114-116.
- Sydney Voice and Swallowing [Internet]. Evaluating Swallowing. Sydney Voice & Swallowing; [cited 2024 June 20]. Available from: https://svas.com.au/swallowing/evaluating-swallowing/
- Beers B [Internet]. P-Value: What It Is, How to Calculate It, and Why It Matters. Dotdash Meredith; [updated 2024 May 9; cited 2024 June 20]. Available from: https://www.investopedia.com/terms/p/p-value.asp
